

ADVERTISEMENT
Filtered By: Lifestyle
Lifestyle
The wayward seed: An ectopic pregnancy
+
Make this your preferred source to get more updates from this publisher on Google.
Women Talk
The hospital call came at around 2 a.m.: A 23-year-old patient was at the Emergency Room because of severe abdominal pain which started a couple of hours ago. She was doubled up, with clammy, cold hands, and pale. Blood pressure was very low, and her cardiac rate was too fast: 120 beats/min. Her abdomen was tender (painful even when slightly pressed), and an internal examination elicited exquisite pain. She had missed her menstrual period for that month, and her pregnancy test was positive. An emergency pelvic ultrasound confirmed our diagnosis: An ectopic tubal pregnancy.
The hospital call came at around 2 a.m.: A 23-year-old patient was at the Emergency Room because of severe abdominal pain which started a couple of hours ago. She was doubled up, with clammy, cold hands, and pale. Blood pressure was very low, and her cardiac rate was too fast: 120 beats/min. Her abdomen was tender (painful even when slightly pressed), and an internal examination elicited exquisite pain. She had missed her menstrual period for that month, and her pregnancy test was positive. An emergency pelvic ultrasound confirmed our diagnosis: An ectopic tubal pregnancy.
Normally, fertilization of the mother’s egg by the father’s sperm occurs in the distal third of the fallopian tube. The fertilized ovum then swims into the uterus through the tubes, aided by gentle but rhythmic movements of very fine hairs called cilia. The fertilized ovum grows and multiplies into a many-celled hollow structure as it travels, then implants into the endometrium, the inner lining of the uterus. 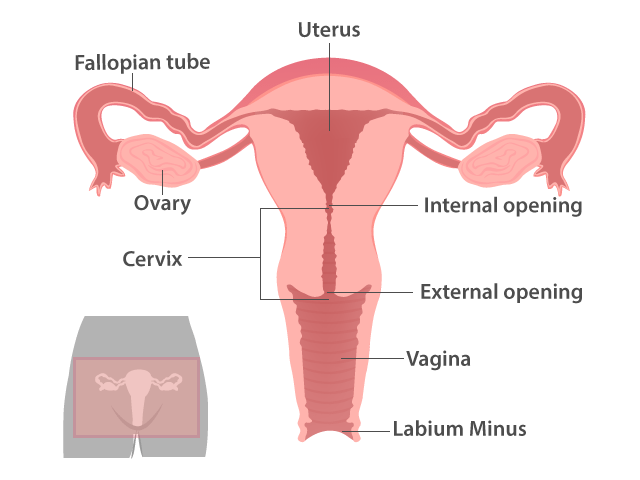
There, the developing embryo puts out branching “roots” of blood vessels to tap and connect with the mother’s blood vessels for nutrition and oxygen (think of a young sapling slowly growing more and more roots into the soil to get all the water and nutrients that it needs for growth). This attachment to the maternal life-giving portion will later develop into the placenta, a disc-like structure where exchange of food and oxygen between mother and child occurs. In a way, the mother’s system accepts this “parasite” that grows within her, a small life that is entirely dependent on her for survival in utero.
In ectopic pregnancy, the seed somehow loses its way. “Ectopic” literally means “outside,” and ectopic pregnancy means a pregnancy that occurs outside the womb or uterus. The most common site for this are the fallopian tubes (tubal), ovaries, abdomen, or even the cervix.
Why does this happen? There are still no definite answers. Some authors theorize that any previous condition that causes distortion of the tube could retard the swimming back of the fertilized ovum on time. A previous infection can cause narrowing of the diameter of the tubal lumen (hole). This smaller diameter may allow the sperm to pass through in its search for the egg, but after it does, the fertilized ovum, which is larger, could no longer pass through on its way to the uterus. This delay would give time for the fertilized ovum to grow “roots” within the tube, tap the maternal vessels, become “fixed,” and grow.
A condition called endometriosis, where uterine glands are found abnormally in places where they shouldn’t be, like the tubes, increases the receptivity of the tubal lumen for implantation. Anatomical distortions of the tube (kinking, previous surgeries that could cause adhesions) could also lead to tubal pregnancies.
These hypotheses however could not explain other ectopic pregnancies: abdominal, ovarian, and cervical. For indeed, after fertilization, it is possible that the fertilized egg, instead of going into the uterus, becomes extruded out into the peritoneal (abdominal) cavity through the distal ends of the tubes, and implants on surfaces that are hospitable to it. Again, it will grow its “roots” for survival, whether this is on the abdomen, ovaries, or even the cervix.
The most common however, is tubal pregnancy. The fallopian tubes have different parts: some are narrow and some, wide. A part of the tube is also embedded into the “horns” of the uterus itself. Within the tubes are rich plexuses of blood vessels, immediately tapped by the ectopic pregnancy for survival. Very soon, their circulations become one.
Because the tube is not wide enough for the growing embryo, the mechanical pressure of the burgeoning mass and the invasiveness of its blood vessels will cause rupture of the tube. This is of course, a catastrophic event, like the patient described above. Hemorrhage will occur inside the abdomen, and she will lose a lot of blood.
Sometimes, when the fertilized ovum implants near the end of the tube, it simply becomes detached (called tubal abortion) because the tube could no longer support it. Bleeding also occurs from where it was implanted, but not as profuse as if it were inside the tube. Many times too, tubal pregnancies occur without being detected, the fertilized ovum dies out because of lack of nutrition, and simply gets “buried” inside the tubal lining. Only later (as histopathlogical specimens) could they be detected as smooth (“hyaline”) area seen under the microscope. Some ectopic pregnancies might also be luckily diagnosed while they are unruptured. In these cases, early surgery is life-saving.
Because a ruptured ectopic pregnancy is life-threatening, there is a need to stop the internal bleeding immediately. When one gets a positive pregnancy test and abdominal pain occurs, it is best to consult a doctor. It could simply be threatened abortion, or even acute appendicitis (which also needs surgery), kidney stones, or even gallstones. Advances in pelvic ultrasound too, make the diagnosis of an ectopic pregnancy easier. Women nowadays, whether married or not, also easily admit to having sexual intercourse, and this is a great help in the diagnosis.
Inside the abdomen, the ruptured blood vessels are immediately identified and clamped. Blood for possible transfusion(s) is often needed. If conserving the tube is a concern for future pregnancy, the surgeon might opt to leave the tube open, after securing the bleeders. Or, she may choose to close the tubal defect with sutures. Removal of the whole tube (salpingectomy) is rarely done now especially for young patients who are still desirous of pregnancy. Some surgeons, adept at laparoscopic surgery, might manage the ectopic laparoscopically, whether ruptured nor not.
Will ectopic pregnancies recur? If we think of the possible reasons for ectopic pregnancies (previous pelvic infections, endometriosis, etc) these would still be present even after the surgery. So prevention of pelvic infections and active treatment for endometriosis might help; also removal of adhesions if present, during surgery.
The key in ectopic pregnancy is a high index of suspicion. In our patient, we found a ruptured tubal ectopic pregnancy, about seven weeks old, did a salpingotomy (we sutured the bleeders and left the small defect open), but we needed to transfuse blood. She recovered well, and went home recovered, on the fourth post-operative day. —KG, GMA News
Alice Sun-Cua is an author and practicing obstetrician-gynecologist at the San Juan de Dios Hospital in Pasay City.
Illustration by Analyn Perez, GMA News
Illustration by Analyn Perez, GMA News
