

ADVERTISEMENT
Filtered By: Lifestyle
Lifestyle
Women Talk: Myomas—what are they, really?
Lotlot, a 27-year-old housewife with three children, came to see me because of pain she was feeling in her lower abdomen. She noted some discomfort during sexual intercourse lately, as well. Her menses were regular, with no dysmenorrhea. Upon examination, I discovered that there were growths in her uterus, making the whole organ larger than normal; and on ultrasound, these were confirmed to be fibroids, or myomas.
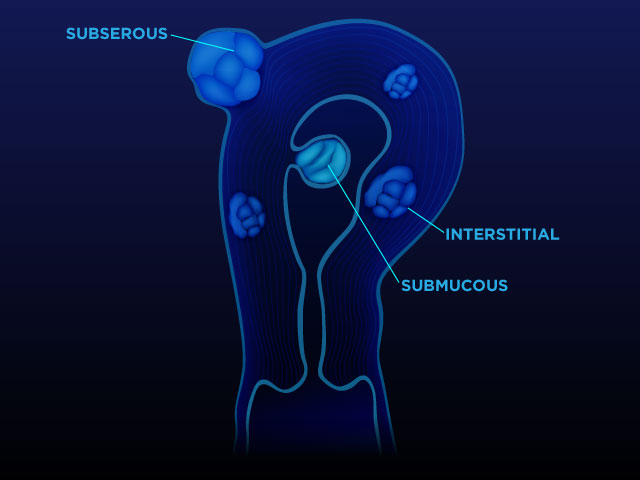
Myomas are benign, solid tumors growing out from the muscular layer of the uterus. These could grow out into the surface of the uterus (subserous type), or simply stay within the muscular layer (interstitial or intramuscular), or grow into the uterine cavity (submucous). Some have stalks (pedunculated). All of these will make the uterus, essentially a muscular organ, grow larger, usually with an irregular shape.
If these myomas are small, there is no need to worry too much about them. Small means measuring less than 4 centimeters—but this is arbitrary, as the location of the myoma and not its size will sometimes make the difference in the management. Because myomas are estrogen dependent, we expect them to grow, even slowly, throughout the life of woman in the reproductive age.
For myomas, then, there is room for cautious waiting if the tumors are not large. However, there are indications for its surgical removal, and these include:
- (1) Pain. The enlargement of the fibroids could cause cramping or frank pain in the lower abdomen. Many times, painful menstruation develops, and even pain during sexual intercourse.
- (2) Bleeding. Because myomas, especially the submucous ones, increase the area of the uterine lining, there will be more areas from which menstrual bleeding could come from. Myomas then may cause heavy menstruation, and loss of too much blood may lead to anemia. Gynecologists though, know that changes in menstruation could be caused by the presence of myoma/s, but in most cases, they would first want to rule out other causes of menstrual irregularities, even with the presence of myoma/s. This is because the bleeding could be due to something else. An endometrial biopsy is usually first done before attributing the bleeding to the myoma.
- (3) Urinary symptoms. Because of mechanical compression of the bladder (which is just anterior to the uterus), some urinary retention could follow in large myomas.
- (4) Bowel irregularities. Like the urinary symptoms, myomas could grow posteriorly and also compress the rectum, and bowel irregularities may ensue.
- (5) Infertility. There can be anatomical distortions of the pelvic organs by the fibroids, which could lead to difficulty in conception.
- (6) Sudden growth. Benign myomas are slow growing. They take years to grow; if there is sudden increase in size, a suspicion of a malignancy arises, and proper work-up of the patient is needed, with the help of a gynaecologic oncologist.
- (7) A large, benign fibroid, especially in small, thin women, could grow to such a large size, distending the abdomen. This is unacceptable for many, for cosmetic reasons.
What are the options, then, when myomas are present? As mentioned, if they are asymptomatic and not large, a regular gynaecologic check-up and pelvic ultrasound (or MRI) may be made to monitor the size of the growths. Some myomas simply stay the same and never grow until the woman reaches menopause, where, theoretically, because hormones have ebbed, the fibroids will no longer grow bigger.
If surgery is opted for, one can have a more conservative myomectomy—that means removing the myoma/s only. Patients who are young and still desirous of pregnancy may be offered this option. The surgery may be done through laparoscopy, or open surgery.
There are instances, though, where very tiny myomas lie in wait among the muscles and later grow into larger ones as well. So the removal of the myomas will not be a 100% guarantee of being myoma- free throughout life.
If the symptoms are severe, where the woman suffers greatly from abdominal pain, profuse menses, and she is satisfied with the number of her children, an abdominal hysterectomy may be done—this means the removal of the entire uterus. Removing the ovaries will be at the discretion of the gynecologist. If the ovaries are retained, the woman will no longer have her monthly menstruation, but will still have functioning ovaries that will serve her well until menopause. So having a hysterectomy does not necessarily mean no circulating hormones, which are necessary for many metabolic functions.
For the past few years, GnRH (hormones) have been introduced not only for some hormonal problems in women, but also because it “shrinks” uterine myomas. Its use has been advised in very large myomas to make them smaller; which means a less bloody surgery (remember that myomas have big blood vessels which contain large amounts of blood as well), a faster intra-operative procedure, and less exposure to anesthetics. GnRH drugs are injected intramuscularly every 6 months, but have notorious side effects like vasomotor symptoms (hot flushes not unlike menopause) and osteoporosis (bone loss), so these cannot be used forever.
In Lotlot’s case, she had three myomas, the largest of which was 7.5 cm. Was she still interested in having more children? She said yes, her husband still wanted to try for a girl, as all three kids were boys.
The location of the largest myoma was also crucial: it was in the lower uterine segment, the area where the baby’s head comes down during labor and delivery. And because myomas were hormone-dependent, they could grow larger in the course of a pregnancy. I advised a myomectomy, which is a surgical removal of the myomas, leaving the uterus and ovaries behind.
The surgery was successfully performed, and after an uneventful post-operative course, she went home after four days.
Lotlot and her husband have been advised, however, to wait for at least a year before attempting to have another child to allow the wounds in the uterus to heal. — VC, GMA News
Dr. Alice M. Sun-Cua is an author and practicing obstetrician-gynecologist at the San Juan de Dios Hospital in Pasay City.
Lotlot and her husband have been advised, however, to wait for at least a year before attempting to have another child to allow the wounds in the uterus to heal. — VC, GMA News
Dr. Alice M. Sun-Cua is an author and practicing obstetrician-gynecologist at the San Juan de Dios Hospital in Pasay City.
